You are here: Professional > Interpretation
Reactions to TRUE Test® should be read 72 to 96 hours after application. This time span is necessary for allergic reactions to develop fully and for irritant reactions to subside. Readings at 48 hours are preliminary and should be confirmed definitively at 72 to 96 hours. Reference 14
Neomycin sulfate and p-phenylenediamine (PPD) sometimes cause late reactions that appear 4 to 5 days after application. Patients should be instructed to report these. If appropriate, an additional office visit will verify a late reaction. Reference 14
It is important to note that PPD may turn the allergen test area black on some patients. This is because the allergen is a dye; it does not represent an allergic reaction. This discoloration may remain for up to 2 weeks. Reference 14
An identification template is provided for quick identification of any allergen that caused a reaction. To ensure correct positioning, marks on the skin should correlate with the notches on the template. Reference 14
The identification template supplied with TRUE Test® ensures accurate identification of the allergen patch responsible for a given reaction.
Interpretation of reaction sites is based on the method recommended by the International Contact Dermatitis Research Group. Reference 20
It is important to note that skin tone affects the appearance of test results. Interpretation Key Based on Recommendations by the International Contact Dermatitis Research Group.

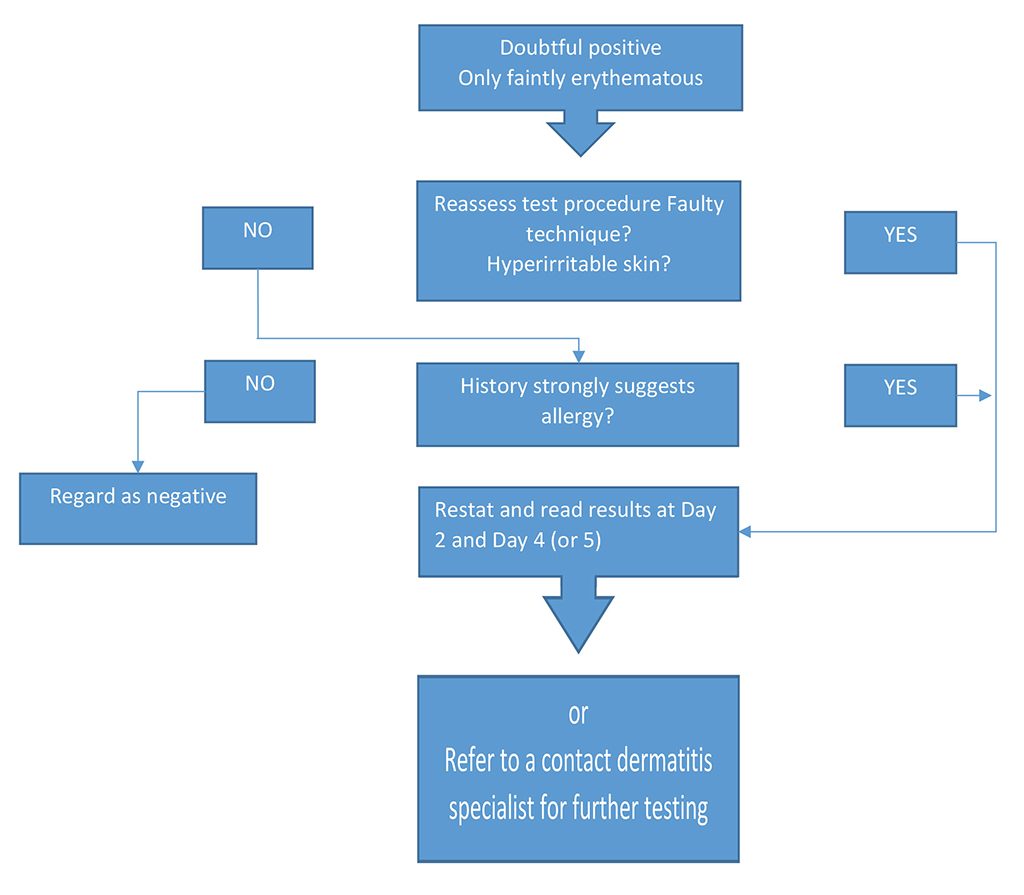
Doubtful reaction
Faint macular or homogeneous erythema, no infiltration
= ?

Extreme positive reaction
Coalescing vesicles/bullous reaction
= +++
Weak positive reaction
Erythema Infiltration Discrete papules
= +
Irritant reaction of different types*
= IR
Strong positive reaction
Erythema Infiltration Papules Discrete vesicles
= ++
Negative reaction
= Not Tested
*Discrete patchy erythema or homogeneous erythema without infiltration, patchy follicular erythema. Petechiae and follicular pustules are usually irritant and do not normally indicate allergy. It is sometimes very difficult to distinguish between an irritant reaction and a very weak positive reaction. Retesting may be necessary to certify contact allergy. Patients who show a negative reaction to the allergens may be sensitive to substances other than those tested. Testing with complementary substances may be indicated.
The majority of extreme positive reactions (+++) and strong positive reactions (++) reflect true positives. With weak positive reactions (+), there is a greater possibility that the reaction will not reflect a true-positive result.
For any true-positive reaction, the patient should be advised to avoid future allergen exposure. The relevance of true-positive reactions to current eruption and/or past allergen exposure must be confirmed with respect to
– the nature and distribution of the skin eruption;
– the validity of the relationship between allergen and recent exposure; and
– patient history, especially of allergic reactions.
Reactions that cannot be explained may be due to
– incomplete history;
– exposure to unsuspected, undetected, or unrecognized allergens;
– the ubiquitous nature of some allergens;
– cross-reactivity; or
– low environmental exposure to an allergen prior to testing.
With reactions of past or current relevance, detailed advice on avoiding the discovered allergen should be given to the patient.
For more information about the allergens on the panels for TRUE Test®, see the Allergen Components page and Patient Information Cards on this site.
Where the relevance of a reaction is unknown and further detailed questioning of the patient fails to disclose the reaction’s significance, the patient should nevertheless be advised to avoid the allergen in the future.
Advice on job changes should be given with extreme caution. Patients sensitive to chromates, for example, do not always improve on changing employment.
Results Negative test results narrow the scope of clinical investigation by indicating that the patient is not sensitive to the allergens that cause up to 80% of ACD. Reference 3
When negative test results are obtained, physicians should consider other possibilities, such as other potential allergens, irritant reactions, or contact urticaria, especially if the hands are involved. Depending on the patient’s history, consideration should be given to referring the patient to a regionally or nationally recognized contact allergen expert for further testing.
– Narrow the scope of clinical investigation.
The patient is not allergic to the allergens that cause up to 80% of ACD False Negatives
– Provide further direction in the pursuit of a diagnosis.
Consider other allergens
Consider irritant reactions
Consider contact urticaria, especially if the hands are involved
– Reassure the patient that his or her condition is not caused by the allergens that most commonly cause ACD
– Minimize the need to restrict the use of products that contain the allergens in TRUE TEST.
A patient with true-negative reactions should be reminded that negative test results occur in 25% to 60% of all cases tested. They should be advised that negative test results provide valuable information that helps in the diagnosis of his or her condition. The patient should be reassured that his or her condition is not caused by the allergens that most commonly cause ACD, which therefore minimizes the need to restrict use of products that contain the allergens in TRUE Test®. It is important to review the patient’s topical regimen, discuss potential irritants/allergens, and suggest alternatives to products that may be causing irritant or allergic reactions or contact urticaria. Patients should be encouraged to contact their physician if they suspect a given product of causing a reaction.
– Tell the patient that negative results are obtained in 25% to 60% of all cases tested.
– Emphasize that negative test results provide valuable information that helps you diagnose his or her condition and initiate treatment.
– Tell the patient that TRUE Test® is designed to identify the allergens that cause up to 80% of ACD.
– Tell the patient that negative test results minimize the need to restrict usage of products that contain the allergens in TRUE Test®.
– Review the patient’s topical regimen, discuss potential irritants/allergens, and suggest alternatives to products that may be causing irritant or allergic reactions or contact urticaria.
– Encourage the patient to contact you if he or she suspects a product of causing a reaction.
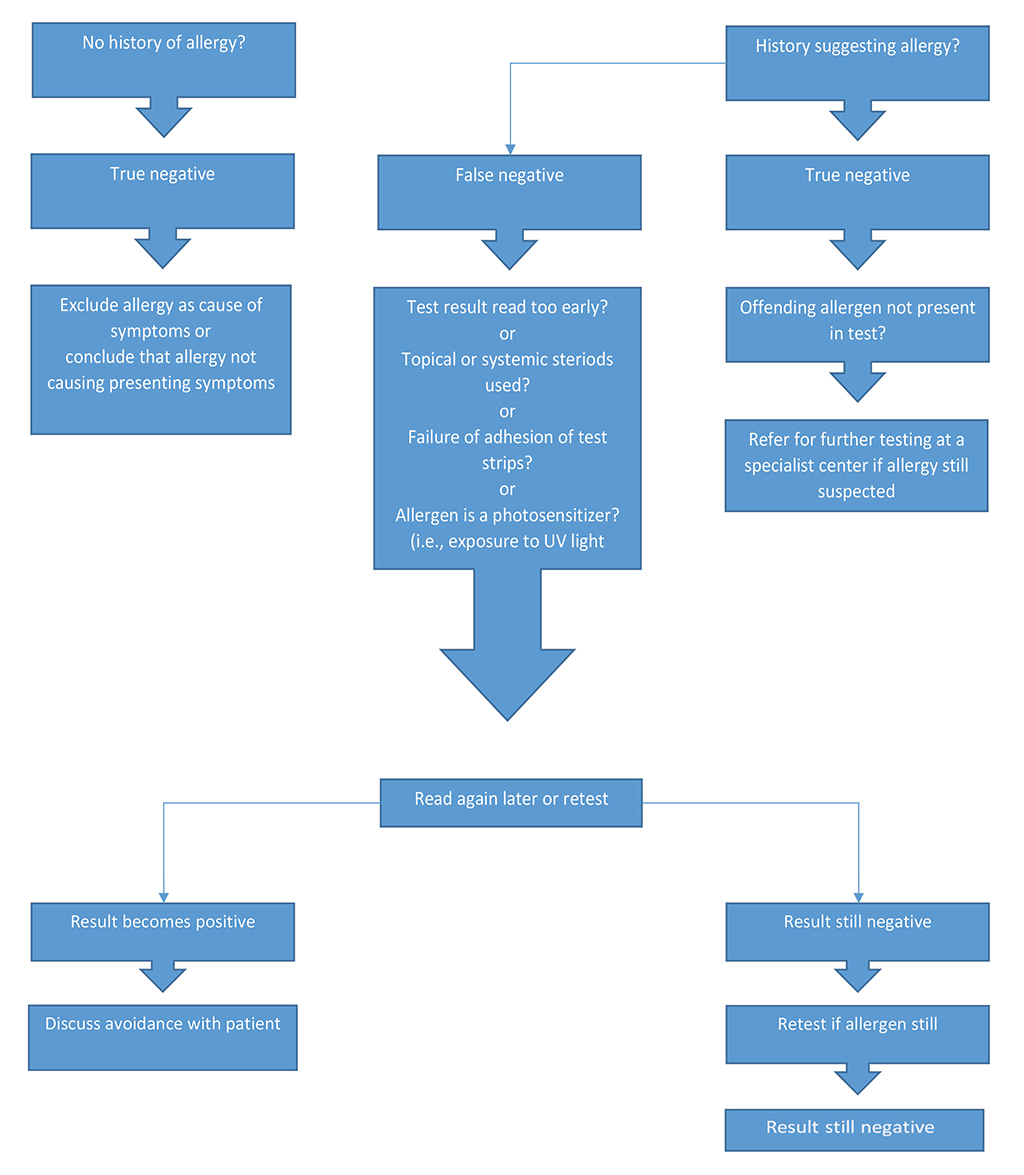
TRUE Test® requires no preparation and consists of standardized amounts of allergens or allergen mixes. The specific composition and concentrations of the test substances and the nature of the vehicles used in TRUE Test® minimize the risk of false negatives. However, the concentrations may occasionally be too low to elicit a positive reaction in weakly sensitized patients, and this can produce a false-negative result.
False-negative reactions may occur for several other reasons. Some positive allergic reactions only appear on the third day or later. If TRUE Test® is read before 72 hours, allergic reactions will have had insufficient time to develop fully and may appear negative. False negatives also may occur if the patient used topical corticosteroids on the test site or took oral corticosteroids equivalent to 15 mg of prednisolone within 2 weeks prior to the test. (Topical steroids on nontest areas may be appropriate.)
False-negative reactions can also occur if there is insufficient contact between the allergen patch and the patient’s skin, or if the test site did not remain dry throughout the testing period.
Other causes of false negatives include
– absence of UV light for photosensitizing allergens;
– absence of adjuvant factors involved in eruptions; and
– correct allergen not tested
If reactions are negative or doubtful but history strongly suggests allergy, consideration should be given to referring the patient to a regionally or nationally recognized contact allergen expert for further testing.
The safety and efficacy of repetitive testing with TRUE Test® are unknown. Sensitization or increased reactivity to one or more of the allergens may occur. The benefits of repeat testing should therefore be evaluated carefully against the possible risks. In addition, the safety and effectiveness of TRUE Test® in children have not been established.
If doubtful or minimal reactions occur, the timing of the reading should be checked. Some allergens may show positive reaction only on the third day or later. Most doubtful reactions should be regarded as negative or the allergen test should be repeated.
Characteristic | Allergic reaction | Irritant reaction |
| timing | Trends to persist or become more market from Day 2 to Day 4; may only appear after Day 2 | Tends to be maximal by Day 2 and fade on patch removal |
| outline | Tends to spread | Often sharply delineated |
| lesion | Usually palpable and eczematous; may be vesicular | May show discrete, patchy erythema; may be follicular or porous, pustular, and bullous |